
System-based thinking (SBT) describes a set of subconscious thought processes aptly named System 1 (S1) and System 2 (S2). S1 is characterized by fast, automatic thinking, while S2 is slow and activated when critical thinking is necessary. The profession of medicine relies heavily on SBT — the ability to rapidly diagnose, treat, and improvise during stressful situations is dependent on these systems, which develop and mature throughout one’s training. However, frequent exposure, heuristics shortcuts, and intrinsic biases can lead to medical errors and mistakes, making SBT necessary but highly flawed. Consequently, understanding how physicians develop and utilize these systems can minimize inherent errors and improve patient safety.
Although seasoned practioners rely heavily on both types of SBT, medical students undergo a maturation in thought processing, namely the transition from slow to fast thinking. Students new to the wards rely heavily on S2 in order to obtain a thorough history or perform a detailed physical exam. Conversely, interns and residents will have converted these daily tasks to S1 thinking and instead utilize S2 thinking to formulate an assessment and plan, manage acutely ill patients, and lead goals of care discussions. Thus, the cumulative effect of medical training allows for the consolidation of much of our daily responsibilities from S2 to S1 thinking. These subconscious heuristic processes further enable us to provide quality medical care through generalizations, shortcuts, and algorithms for common clinical presentations.
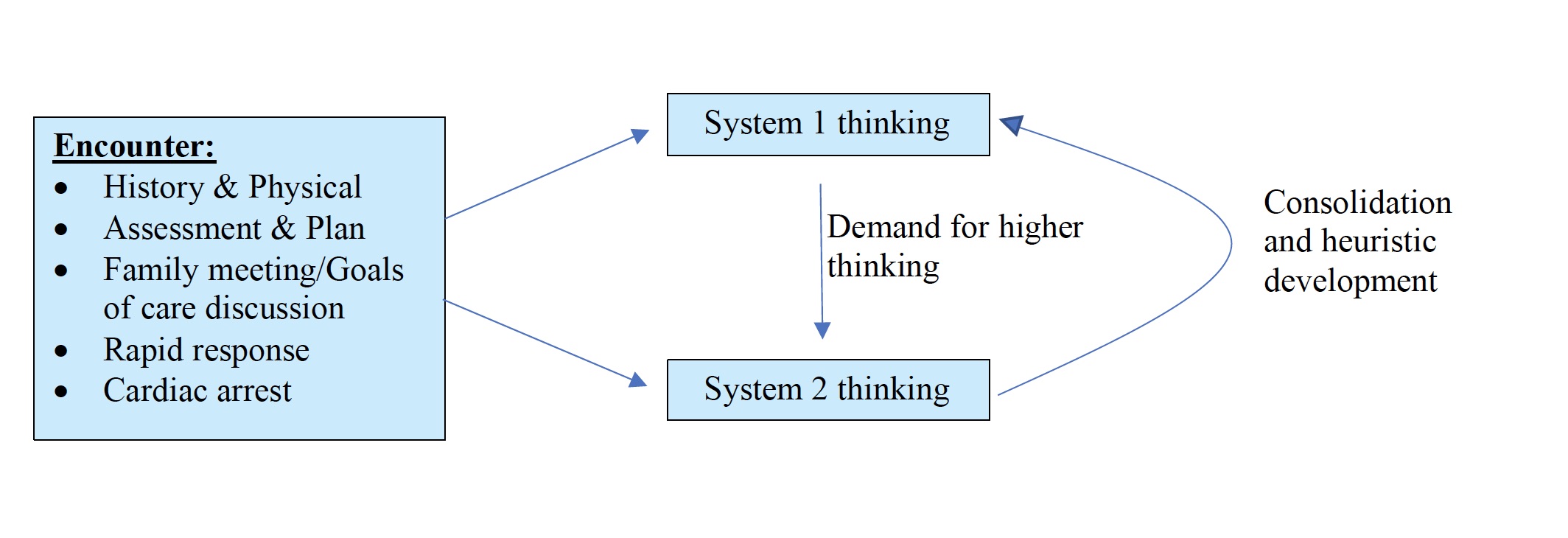
A complex interplay exists between these two types of thinking, as shown in the figure. Sometimes, the workup and diagnosis of a disease is a straightforward and unidirectional process. For example, obtaining a focused history and physical exam using S1 thinking should allow a practitioner to diagnose costochondritis in a young male with chest tenderness reproducible to chest palpation. In other cases, the process might be more convoluted, requiring an interplay between S1 and S2. The acute onset of hypoxic respiratory failure is one such situation. Here, a well-trained practitioner uses S1 to assess a patient’s “ABCs” such as obtaining a full set of vitals, confirming IV access, and initiating supplemental oxygen. Simultaneously, S2 allows for the rapid development of a differential for acute hypoxia including flash pulmonary edema, aspiration pneumonia, or mucous plugging. A mixture of S1 and S2 also enables the practitioner to obtain a 12-lead EKG to rule out acute coronary syndrome, chest radiograph to evaluate for flash pulmonary edema or aspiration, and perhaps an arterial blood gas to confirm hypoxemia. These situations may overwhelm medical students (and even residents) but nonetheless work to consolidate much of our day-to-day thought processing over from System 2 to System 1.
Encounters muddied by vague symptoms, difficult patients, and physician fatigue can accentuate the pitfalls of SBT. Daniel Kahneman, author of Thinking: Fast and Slow, states, “System 1 is gullible and biased to believe, System 2 is in charge of doubting and unbelieving, but System 2 is sometimes busy, and often lazy.” This must be kept in mind when evaluating patients with seemingly harmless presentations such as atypical chest pain, in which ACS or pulmonary embolism may be the true culprit. While the transition from S2 to S1 thinking is imperative for a clinician to be efficient and successful, we must realize that the heuristics we use and the biases we hold can lead to significant error. In fact, the United States battles approximately 400,000 annual preventable deaths.
Opportunities exist throughout a physician’s training to promote critical thinking, combat bias, and prevent medical error. This process should begin in the adolescence of training: medical school. Students frequently study zebra cases, rare and infrequently encountered disease states, but less stress appears to be placed on abnormal presentations of common diseases. Instead, have students recognize that uncontrolled hypertension may be the result of medication non-adherence from unaffordability, frequent dosing schedules, or embarrassing side effects, and not from a primary hyperaldosteronism or renal artery stenosis. The use of S2 may result in a medical student arriving at the correct diagnosis, while S1 alone may lead to an unnecessary, expensive, and potentially invasive workup.
In residency, our success and efficiency are the result of experience, heuristic shortcuts, and confidence, all significantly related to improved S1 and S2 functionality. Bedside rounds allow for an intern to obtain a pointed history, perform a less practiced exam technique, or lead a difficult end of life discussion. Interns and residents should be challenged to create a list of differential diagnoses not initially considered. Perhaps a patient’s poorly controlled, recurrent asthma exacerbations are actually secondary to acute bronchopulmonary aspergillosis. Maybe the unilateral lymphedema of a well-traveled patient is caused by lymphatic filariasis and not deep vein thrombosis or venous insufficiency (though they should be ruled out). Discussing the possibility of these diagnoses makes rounds more enjoyable, thought provoking, and memorable. Lastly, trainees should have the ability to question their superior’s decisions without fear of repercussion. Even those with the most experience can develop a lazy or preoccupied S2. Most importantly, as human beings, we must realize that we are fallible and destined to make mistakes. Only after recognizing our potential for error can we attempt to optimize our application of System 1 and System 2 thinking.
Resident Physician Contributing Writer
Brown University
David was born and raised in Parsippany, New Jersey. He obtained his Bachelors of Science in Microbiology at New Mexico State University followed by both his Masters in Biomedical Science (MBS) and Doctor of Medicine (MD) from Geisinger Commonwealth School of Medicine. He is currently an Internal Medicine resident at Brown University, where he has invested himself in clinical research regarding coronary and peripheral artery revascularization, He is pursuing a career in interventional cardiology.